Dr Gideon
Sandler
Undescended Testes
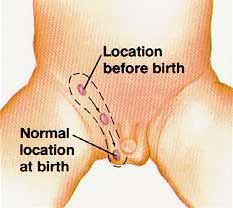
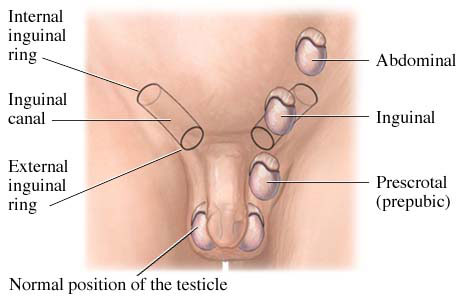
The testis develops near the kidney during pregnancy and drops down to the scrotum before, or sometimes during the first few months after birth. An undescended testis is one that has stopped along the path of descent. It is most frequently stuck in the groin area. The testis may drop during the first 3-6 months, but is unlikely to do so after that time. The testis needs to be in the scrotum where is it a little cooler than the rest of the body for it to develop and produce sperm normally when the boy grows older.
How is undescended testis treated?
Undescended testis is treated with an operation in which the testis is located and brought into the scrotum. The operation for undescended testis is ideally performed between 9-12 months of age. If the testis is located in the groin, the operation is done in one stage. If the testis is located in the abdomen, two separate operations are usually required. The operation is performed under general anaesthesia and takes about 30 minutes. Your child should not have to spend the night in hospital.
Preoperative Preparation
Your child cannot eat for 6 hours before the procedure. In breast fed babies this time may be reduced by the anaesthetist. Your child can drink water for up to 2 hours before the operation. The Day Surgery Unit will instruct you the day before surgery to confirm fasting times. It is useful to bring your child’s favourite toy along on the day.
Anaesthesia
The anaesthetist will meet you and your child prior to the procedure. They will discuss the anaesthetic with you and take you through to the operating theatre. Your child will be anaesthetised using a face mask and then you will be taken to a waiting area. Once your child is asleep a drip is inserted often in the hand or arm, but occasionally it may need to be sited in the leg. Local anaesthetic may be injected into the base of the spine (caudal block). The anaesthetist will discuss this with you.
Procedure
A cut is made in the groin area on the side of the undescended testis through which the testis is found and carefully released. There is often a small hernia which has to be peeled of the blood vessels to the testis and the sperm tube. This usually allows the testis to be placed in the scrotum through a second cut in the scrotum. The testis is fixed with sutures to the inside of the scrotum. The wounds are closed with dissolving sutures. Local anaesthetic is injected during surgery to numbs the area for 4-6 hours. Tissue glue is applied as a dressing. It is lilac in colour and takes 2 weeks to fall away.
In 15-20% of boys the testis is not felt in the groin. In this situation a laparoscopy is performed to locate the testis in the abdomen. If found, an attempt is made to release the testis and drop it to the scrotum. If too high a staged procedure is performed.
Initial recovery
On completion of the operation your child will be taken to the recovery area. Children often initially appear distressed and a little confused upon waking up but will quickly settle down once you are with them and if offered a drink or something to eat. Full recovery usually takes about 2-3 hours after which you can go home.
Post-operative course
Children’s paracetamol should be given for pain relief for 24 hours. After that use paracetamol only if needed. Some children need additional medication such as ibuprofen or celecoxib. Opiate (morphine-type) medications are not usually required. Paracetamol and ibuprofen can be given at the same time and work well together. Follow the dosages recommended on the packaging or by the anaesthetist. Never give more than has been prescribed.
It is quite normal for the scrotum to look swollen and there may be some bruising. This usually resolves in week or so.
In general, your child may eat a normal diet after surgery. Vomiting is common on the day of surgery. It is temporary, and usually due to the anaesthetic and pain-relief medications that are used. If vomiting occurs, start with clear liquids and add solids slowly for the first day.
Return to activity
- Activity: Your child should avoid strenuous activity first 1-2 days. Sport and swimming are best avoided for 3 weeks after surgery.
- School: Your children may return to day care or school when comfortable.
- Bathing/showering: As the wound is waterproof, bathing and showering is safe after the operation.
- Wound care: No specific wound care is required. The stitches are absorbable and do not require removal. No dressing changes, creams or ointments are required.
- Stool softeners and laxatives: May be needed to help regular stooling after surgery, especially if opiates are needed for pain.
Call the doctor’s office if:
- You see any signs of infection: redness along the incision site, increased swelling, discharge
- Your child’s pain gets worse or is not relieved by pain killers
- There is bleeding from the incision
- Your child has an abnormal temperature
- Vomiting continues on the day after surgery
- If you have any other concerns
Follow-up
I will review your child 4-6 weeks after the surgery to ensure healing of the wound. For patients from rural areas this may be deferred to your local General Practitioner or Paediatrician. Please ring soon after the operation to arrange a convenient time.
Complications
This is a common operation with a low complication rate. The vast majority of children who have this operation recover well and have no serious complications of surgery. However, complications can occur. Some of the recognised ones include:
Infection & Bleeding
There is a 1-2% risk of bleeding or wound infection after surgery. The wound will appear red, be tender to touch and may discharge pus or blood. If this occurs, a course of antibiotics may be required, and you should contact me or present to your General Practitioner or Local Hospital as soon as possible.
Damage to Testicular Vessels
There is a <1% chance of damage to the testicular vessels. This occurs more commonly when repairing recurrent undescended testis and may result in loss of function and/or shrinkage or disappearance of the testis over a few weeks.
Damage to the Vas Deferens
There is a <1% chance of dividing or damaging the vas deferens. This tube takes sperm from the testis to the penis during emission and ejaculation. If it is damaged, the testis can be rendered non-functional as a reproductive organ.
Recurrence
There is a 5% chance the testis may not stay in the scrotum following surgery. In this situation further surgery may be required a year later. Occasionally (5%) the testis cannot be brought down in one stage and then a second stage is performed later.
Testicular Cancer
After puberty boys should be instructed to perform testicular self-examination on a monthly basis because of slightly increased risk of testicular cancer in boys with undescended testis. Orchidopexy does not eliminate the risk but makes it easier to detect.
More Information
If you have any questions, please do not hesitate to contact us.
Ph: 02 8307 0977
Fax: 02 8088 7420
Email: info@drgideonsandler.com
Please refer to the following resources for more information:
- Undescended Testes
The Sydney Children's Hospitals Network - Undescended Testes
The Royal Children's Hospital Melbourne - Undescended Testes
Texas Children's Hospital
This page is intended to provide you with information and does not contain all known facts about undescended testes. Treatment may have uncommon risks not discussed here. Please do not hesitate to ask any questions you may have.